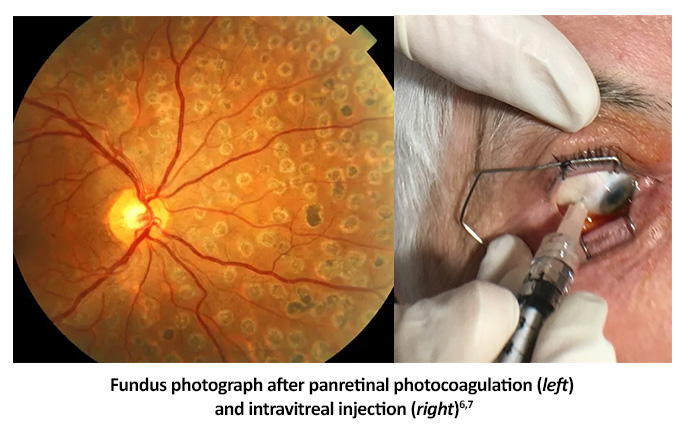
Laser panretinal photocoagulation (PRP)
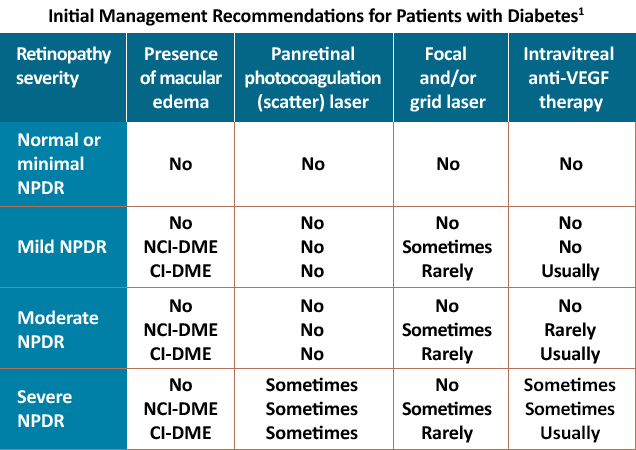
Laser PRP decreases the risk of severe vision loss in people with severe NPDR and high-risk factors such as poor compliance with follow-up, impending cataract extraction or pregnancy, and blind or advanced DR in the fellow eye.1,4 People with very severe NPDR or worse have approximately a 50% chance of worsening to PDR within 1 year.1
Anti-vascular endothelial growth factor (anti-VEGF)
Studies suggest that treating moderate to severe NPDR with anti-VEGF in some people can improve signs of retinopathy and delay progression from severe NPDR to PDR.5,8 The two primary anti-VEGF therapies that are FDA-approved to treat any degree of NPDR are ranibizumab and aflibercept.3 Data from the Protocol S, RISE/RIDE, VIVID/VISTA, and PANORAMA trials show that these anti-VEGF therapies can help eyes with any level of DR, with or without DME.3 Eyes with more advanced NPDR respond particularly well to anti-VEGF therapy, with approximately 80% showing regression of retinopathy severity.3
DME is another facet of diabetic retinopathy that may run a concurrent or independent course with NPDR. It can be a significant source of visual impairment for patients and may need ocular therapy. Focal macular laser was the mainstay of center-involving DME treatment; however, intravitreal anti-VEGF injections have moved to the forefront and are now first-line therapy for DME.9
In addition to ranibizumab and aflibercept, faricimab has been FDA-approved to treat DME (YOSEMITE/RHINE).10,11 Additionally, higher molar concentration aflibercept (8mg) has been FDA-approved for the treatment of DR and DME (PHOTON).12 Some ophthalmologists also use bevacizumab off-label for retinal edema.10
Many patients respond well to anti-VEGF agents, improving 1-3 lines or more on the Snellen vision chart.10 Unfortunately, up to 40% of people experience persistent DME, although, even in these cases, a substantial portion have shown ≥2 lines of improvement in clinical trial settings.10
Alternative treatments
Alternative treatments may be considered if the DME does not respond after 3-6 monthly intravitreal injections.9 Laser therapy may be initiated after 6 months of anti-VEGF treatment. Intravitreal injections or implants of steroids may also improve retinal thickening and visual acuity.10 However, long-term results have not been as promising as either laser therapy or anti-VEGF agents.10